
Ever ponder why a negative blood test feels like the end, even when your body sends mixed signals?

IVF failure is confirmed only by a negative serum β-hCG or clear evidence that implantation didn’t happen. Symptoms like cramping, nausea, fatigue, or light spotting are common but unreliable. These signs often stem from medications or implantation bleeding, not a failed cycle.
If you used ovulation suppression or hormone support, your period will likely start 2–3 days after stopping the meds. In natural-cycle transfers, the period usually arrives on time. Expect your first period after a failed cycle to possibly feel different in flow and length.
📞 Get in Touch for a Free Surrogacy Consultation
📱 +91-8800481100 (WhatsApp | LINE | Viber)
📧 neelam@ivfconceptions.com
Take a short pause before making big decisions. Aim for about a week to emotionally process the result and book a follow-up with your reproductive endocrinologist. Many failures are due to embryonic arrest from chromosomal abnormalities, not uterine issues.
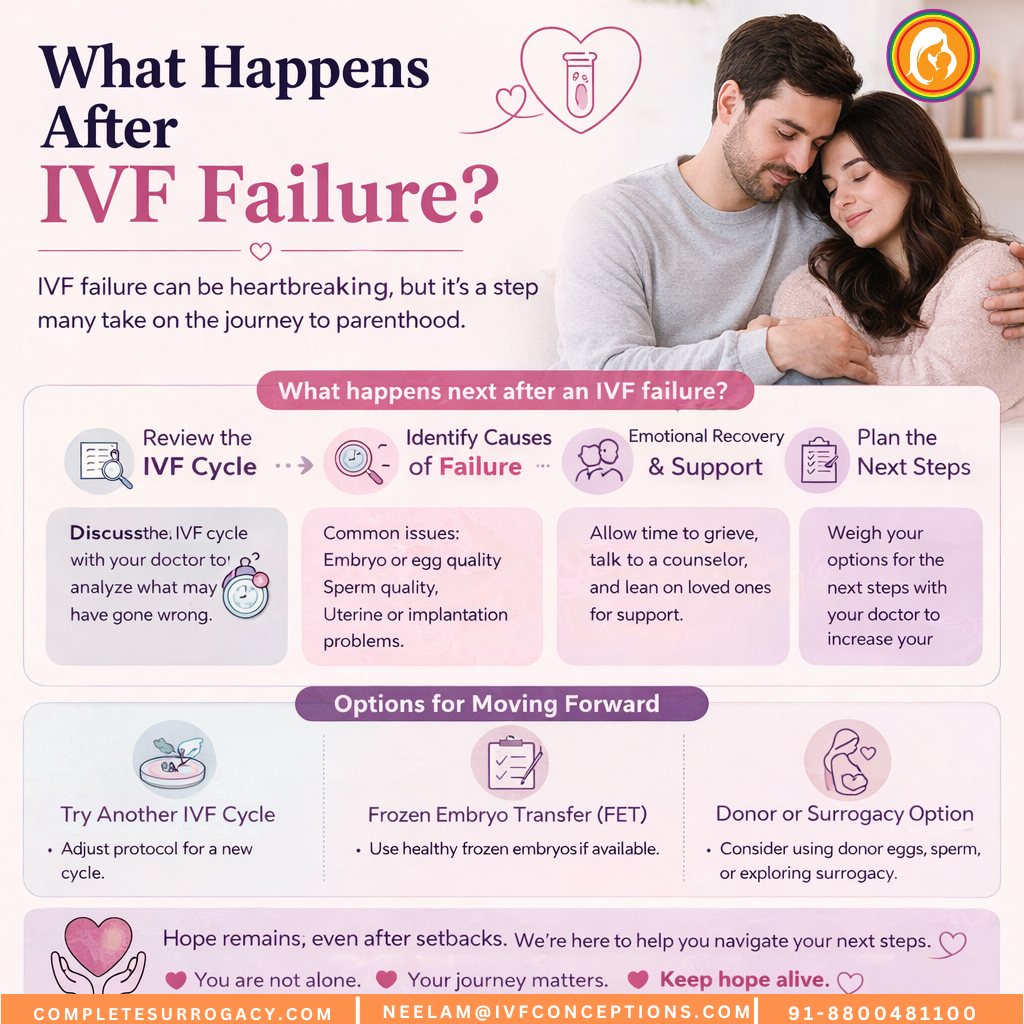
This article explains what happens after IVF failure and outlines practical next steps after unsuccessful IVF. It covers the clinical review your doctor should perform, emotional recovery tips, medical and alternative options, and when to try again. Use this as a roadmap for your failed IVF cycle next steps and to plan a focused conversation with your fertility specialist.
Planning surrogacy abroad?
Read our complete Guide to International Surrogacy to understand the process, costs, legal rules, and timeline for international intended parents.
Additional Resources to Read:
Surrogacy Services in Georgia Country
Surrogacy Services in Colombia
Surrogacy Services in Kazakhstan
Key Takeaways
- The definitive sign of failure is a negative serum β-hCG or clinical confirmation, not symptoms.
- Periods typically return 2–3 days after stopping hormones or on the expected day after natural cycles.
- Take about a week to process the result before making decisions or scheduling next steps.
- Many failures stem from embryonic chromosomal issues, not uterine problems.
- This article will guide your next steps after unsuccessful IVF and how to plan a personalized approach with your specialist.
Understanding What Happens After IVF Failure?
When an IVF cycle ends without a pregnancy, you might feel stunned. This guide explains what your body might show and how emotions often unfold. It helps you take practical steps towards recovery.
Immediate physical signs and what they mean
A negative serum β-hCG or urine pregnancy test confirms no pregnancy. Don’t rely on how you feel. Schedule the β-hCG test on the day your clinic recommends, even if you notice spotting. Spotting can be implantation bleeding and does not always mean failure.
Vaginal bleeding after embryo transfer does not automatically indicate a failed cycle. If bleeding starts, keep taking prescribed medications until your hCG test confirms the result. Call your specialist to report any changes.
Menstrual timing may shift depending on the protocol. In medicated cycles, bleeding often begins 2–3 days after stopping medications. In natural cycles, expect your usual period timing. Your first period after treatment can feel lighter or heavier than normal.
Your ovaries may feel tender after stimulation. If you plan another stimulation cycle, many clinics advise allowing 2–3 months for ovarian recovery. This allows your body to rest and return to baseline.
Emotional reactions you may experience
Shock, emptiness, sorrow, and guilt are common in the first days. You might replay what-if scenarios and blame yourself. These responses are normal reactions.
Treatment fatigue, heightened anxiety, and risk of depression increase after negative results. If your distress becomes severe or lasts beyond a few weeks, seek professional support. This protects your mental health and aids emotional recovery from IVF failure.
Immediate steps that help include letting emotions surface, avoiding major decisions for a short period, and focusing on basic self-care. Regular sleep, balanced meals, and gentle movement support emotional recovery after failed IVF and help stabilize mood.
Practical first steps are simple. Take a brief pause of about one week to rest and reflect. Then schedule a review appointment with your clinic to discuss results. If you feel overwhelmed, look into counseling options to strengthen coping with IVF failure and plan next moves.
| Sign or Symptom | What It May Mean | Practical Action |
|---|---|---|
| Negative β-hCG or urine test | Confirms no pregnancy | Follow clinic instructions, stop or continue meds as advised, book follow-up |
| Spotting after transfer | Could be implantation bleeding or early menstrual flow | Continue medications, record bleeding, inform your specialist |
| Early or altered period | Normal response to hormones or cycle type | Track cycle, note changes, discuss timing with your clinic |
| Ovarian soreness or bloating | Residual effect of stimulation | Rest, light activity, consider 2–3 month recovery before next stimulation |
| Strong emotional reactions | Normal grief, stress, or anxiety linked to loss | Allow time off, practice self-care, seek counseling if prolonged |
Reviewing the Failed Cycle and Identifying Causes of IVF Failure

After a failed cycle, a detailed review is essential to pinpoint the reasons. Begin by summarizing your treatment: the medications you took, the monitoring data, the number of eggs retrieved, and the details of the embryo transfer. This approach helps in planning the next steps and ensures a thorough analysis of the failed cycle.
Clinical review points your doctor should cover
Your doctor should first evaluate how your ovaries responded to stimulation, comparing it to what’s expected for your age and AMH levels. They should also check the medication doses, the number of follicles, estradiol levels, AFC, and any protocol deviations. It’s important to review the egg retrieval process: the number of eggs, their maturity, and any technical challenges.
Next, they should examine the fertilization outcomes and compare IVF and ICSI results. If male factor issues are suspected, sperm analysis is critical. They should also assess embryo development: cell counts on day 3, fragmentation, day 5 blastocyst expansion, and the quality of the inner cell mass and trophectoderm. Requesting embryo images and details on the number transferred and the transfer technique is also vital.
They should also evaluate the uterine cavity using sonohysterography or hysteroscopy, looking for any abnormalities. This includes polyps, submucous fibroids, adhesions, or malformations. Reviewing endometrial thickness and any histology done is also necessary. Confirming luteal support, progesterone levels, and the timing and adherence to medication around transfer is essential.
Laboratory and genetic factors to investigate
High rates of embryo arrest often indicate chromosomal problems. Discuss the possibility of preimplantation genetic testing for aneuploidy (PGT-A) if it’s appropriate for your case. Inquire about the lab’s incubators, media, air quality, and quality-control logs to ensure they meet industry standards. Comparing clinic success rates to those reported by the CDC and SART can help identify any discrepancies.
When fertilization is poor, repeat or expand sperm testing is recommended. Advanced sperm function tests may be necessary if routine semen analysis is normal but outcomes are subpar. If you’ve experienced recurrent implantation failure, discuss targeted tests for endometritis, thrombophilias, or immunologic factors based on your history and risk profile.
After examining embryology and genetics, consider donor options if egg or embryo quality consistently limits success. Your team should outline which issues can be addressed with stimulation changes, lab adjustments, or transfer technique and which require alternative strategies.
Lastly, request a candid, personalized estimate of your chances with a second attempt. Use your age, ovarian reserve, embryo quality, and the expertise of your clinic to guide the next steps and create a realistic plan.
Coping with IVF Disappointment and Emotional Recovery After Failed IVF
After a cycle, the outcome might not meet your expectations. This gap can be deeply unsettling. To navigate emotional recovery after failed IVF, follow specific steps. This approach aids in healing without hasty decisions.
Allow yourself to grieve. Acknowledge your feelings—anger, sadness, or numbness—and give them space. Avoid making major decisions for about a week. This pause helps you think more clearly when planning your next steps.
Practical coping strategies
Reduce stress with evidence-based methods. Try mindfulness, paced breathing, gentle yoga, or progressive muscle relaxation. These techniques can stabilize your mood and reduce anxiety related to IVF failure.
Improve your lifestyle to boost resilience and future fertility attempts. Focus on consistent sleep, balanced meals, moderate exercise, and limit alcohol and tobacco. Keep your BMI between 19 and 30 if planning another cycle.
Prevent “what if” thoughts by focusing on what you can do. Schedule a post-cycle medical review, request lab and embryo reports, and gather clinic success-rate data if considering a new center. Taking concrete steps can help you feel less helpless and support your coping.
Where to get emotional support
Seek Fertility counseling from reproductive mental health professionals. Many fertility centers offer in-clinic psychology units or referrals to therapists experienced in infertility. These specialists understand the unique grief of assisted reproduction and can guide your emotional support after IVF failure.
Join support groups and peer communities to combat isolation. In-person groups, online forums, and local RESOLVE chapters provide shared experiences and coping tools. Therapists with infertility expertise can help set boundaries with family and partners.
Discuss how and when to share details with your partner and family. Ask them to respect your boundaries and avoid intrusive questions until you’re ready. Clear communication helps preserve relationships and aids in recovery.
If you experience severe depression, suicidal thoughts, or can’t function, seek immediate help. Use crisis lines, your primary care doctor, or emergency services. Clinics often provide referrals to psychologists and social workers familiar with IVF grief.
| Action | Why it helps | When to do it |
|---|---|---|
| Allow 1 week to grieve | Prevents rushed decisions and reduces regret | Immediately after test results |
| Request cycle reports and embryo photos | Provides concrete data for clinical review | Within 1–2 weeks post-cycle |
| Begin short daily mindfulness | Lowers anxiety and improves sleep | Start within days and continue long term |
| Consult reproductive mental health specialist | Offers targeted therapy for IVF-related grief | When emotional distress interferes with daily life |
| Gather clinic success-rate data | Helps assess options and inform next steps | Before deciding on a new clinic or repeat cycle |
Next Steps After Unsuccessful IVF: Medical and Practical Options
After a failed cycle, you have several options to consider. Begin with a detailed clinical review to determine if another attempt at IVF is advisable. This review should examine various factors such as stimulation response, egg and sperm quality, embryo development, lab techniques, and uterine health. The insights gained will guide your medical and practical planning for the next step.

For those contemplating another IVF attempt, small adjustments to the protocol can significantly enhance success rates. Personalize the ovarian stimulation drugs and doses based on your previous response. Consider blastocyst culture and single embryo transfer when the embryo quality is high. Ensure proper progesterone levels before transfer and adjust luteal support as needed.
Genetic testing with PGT-A can be beneficial, reducing implantation failures, mainly for those with advanced maternal age or recurrent loss. Use ICSI or advanced sperm selection when male factor issues are suspected. In some cases, assisted hatching may be necessary if the zona pellucida seems resistant to implantation.
Lab quality is critical. If concerns arise about embryology technique or clinic success rates, switching to a center with better SART or CDC outcomes can make a significant difference. Discuss the timing of your next cycle; many clinics recommend a 2–3 month gap to investigate causes and support ovarian recovery. A frozen embryo transfer can proceed sooner if embryos are already cryopreserved.
Alternative fertility treatments after ivf should be considered when repeat cycles fail or when egg quality is a concern. Donor eggs or embryos can offer high success rates for those with poor oocyte competence or diminished reserve. Gestational surrogacy is an option when carrying a pregnancy is unsafe or not possible.
Frozen embryo transfer (FET) is a gentler option that avoids new stimulation. Intrauterine insemination (IUI) may be suitable for some diagnoses but generally yields lower success rates than IVF. It’s not usually recommended immediately after a failed IVF unless the underlying diagnosis changes.
Improving IVF success rates can be achieved by addressing modifiable health factors. Optimize your weight, stop smoking, treat uterine issues like polyps or endometritis, and manage thyroid or metabolic problems. Be cautious with experimental immune or anticoagulation treatments; use them only when evidence supports their use for your situation.
Use the table below to compare common next-step options, likely benefits, and typical considerations to help you weigh choices when trying again after unsuccessful ivf or exploring alternatives.
| Option | Potential Benefit | When to Consider |
|---|---|---|
| Repeat IVF with protocol changes | Improved egg yield or embryo quality through tailored stimulation and lab adjustments | Prior poor response or modifiable lab/stimulation factors; you’re emotionally ready to try again |
| PGT-A testing | Reduces risk of transferring aneuploid embryos; may lower implantation failure rate | Recurrent implantation failure, advanced maternal age, or multiple miscarriages |
| Frozen Embryo Transfer (FET) | Avoids fresh stimulation; allows controlled uterine preparation | Available cryopreserved embryos or a desire to avoid another stimulation cycle |
| Donor eggs/donor embryos | Significantly higher live birth rates when oocyte quality is limiting | Poor oocyte quality, very low ovarian reserve, or repeated failed cycles |
| ICSI or advanced sperm selection | Improves fertilization when the male factor contributed to failure | Poor fertilization in the prior cycle or identified sperm defects |
| Gestational surrogacy | Enables pregnancy when carrying is unsafe or impossible | Uterine factors, major health risks with pregnancy, or repeated uterine implantation failure |
| IUI | Less invasive and lower cost than IVF | Mild infertility causes where IVF may not be immediately necessary |
| Health optimization and targeted treatments | Can boost embryo competence and implantation environment | When lifestyle, uterine pathology, or medical comorbidities are identified |
Deciding When to Try IVF Again and Setting Realistic Expectations
After a failed cycle, you face choices about timing, strategy, and support. Deciding when to try IVF again involves clinical findings, emotional readiness, and practical limits like cost and time. A clear, data-driven path helps you weigh options without rushing.
Review key factors that affect a repeat attempt. Age and ovarian reserve shape baseline odds. Results from your last cycle — egg yield, fertilization, and embryo development — give direct clues. Male factor issues change the approach to sperm testing and ICSI. Uterine anatomy and endometrial health can determine whether transfer timing or surgery is needed.
Clinic quality matters. Look at SART and CDC reports for lab performance and live birth rates. If embryonic arrest was high, consider genetic testing or donor egg options. When to try IVF again often ties to whether modifiable issues exist and how quickly you can address them.
Factors that influence your chances on a second try
Review objective measures first. AMH and AFC signal egg quantity. Prior oocyte yield and embryo grades show how your body responded to stimulation.
Sperm analysis and advanced semen testing reveal male contributors. If sperm quality limited fertilization, ICSI or sperm retrieval methods may improve outcomes. High embryo arrest rates point to chromosomal problems and make PGT-A or donor egg a serious option.
Uterine factors deserve attention. Polyps, fibroids, hydrosalpinx, or chronic endometritis reduce implantation odds. Treating these issues before trying again often raises success rates.
Creating a personalized plan with your fertility specialist
Ask your reproductive endocrinologist for an honest, age-stratified estimate of success for a repeat cycle. Request full cycle records: medication logs, lab reports, embryo images, fertilization tables, and transfer notes.
Work through protocol changes with your team. Possible steps include a different stimulation protocol, PGT-A testing, altered transfer timing, or switching clinics with stronger lab metrics.
Set practical limits. Decide how many attempts you will pursue, a budget range, and trigger points for donor egg or adoption. Plan timelines: a typical wait before a new stimulation cycle is 2–3 months though frozen embryo transfer can proceed sooner.
| Decision Point | What to Review | Typical Action |
|---|---|---|
| Low AMH / poor response | AMH, AFC, prior oocyte yield | Adjust stimulation, consider donor egg if low success odds |
| High embryo arrest | Embryo development rates, grading | Offer PGT-A, consider donor egg or lab change |
| Male factor infertility | Comprehensive semen analysis, DNA fragmentation | Use ICSI, surgical sperm retrieval, or male treatment |
| Uterine issues | Ultrasound, hysteroscopy, endometrial biopsy | Surgical correction, antibiotics for endometritis, optimize lining before transfer |
| Clinic performance concerns | SART and CDC success rates, embryology lab feedback | Compare clinics, request lab-specific data, consider transfer at higher-performing center |
Include mental health and financial planning in your strategy. Work with your fertility team, embryologist, and a therapist to create a realistic timeline. Clear steps make trying again after failed ivf a measured, informed choice, not an emotional reaction.
Conclusion
After a failed cycle, the first step is clear: confirm β-hCG results and take a compassionate pause. Then, plan a detailed review with your reproductive endocrinologist. This review will cover stimulation, egg retrieval, fertilization, embryo development, and transfer technique. It will also examine uterine factors and lab quality.
This audit is key to shaping your next steps after unsuccessful IVF. It turns uncertainty into practical choices. Many failures are due to embryonic chromosomal issues, making personalized decision-making critical.
Discuss options like adjusting protocols, PGT-A, transferring at blastocyst stage, or switching clinics or labs. If you’re thinking of trying again, ask for cycle records and embryo reports. Also, get realistic success estimates based on your data.
Caring for your mental health is essential. Use in-clinic psychology resources, licensed therapists, and peer support to cope with IVF failure. Prioritize self-care and avoid self-blame. Create an emotional and financial plan before moving forward.
For practical next steps, schedule a post-cycle consult and review SART/CDC clinic statistics. Map a tailored medical plan that aligns with your values. With careful review, data-driven changes, emotional support, and realistic expectations, many succeed after an unsuccessful IVF attempt.
Make decisions based on objective records, your priorities, and your specialist’s recommendations. This will guide you on the most informed path forward.
💫 Why Intended Parents Choose Complete Surrogacy for a Safe, Smooth & Successful Surrogacy Journey:
🌍 Access to multiple surrogacy destinations with 15+ years of international experience
🏥 Partnerships with top-tier fertility clinics and agencies, backed by references from past clients
👩🦱 Diverse egg donor options: Asian, Caucasian, African, Oriental, and more
💸 Transparent and affordable pricing—direct payments with no extra agency fees
🔒 No hidden costs—all charges are agreed upon upfront
🤝 Dedicated case manager for personalized support
📲 Fast, honest, and clear communication throughout
📑 Full legal support for visas, documentation, and baby exit processes
🚚 Assistance with frozen sperm/embryo shipment logistics

FAQ for What Happens After IVF Failure?
What is the only reliable evidence that an IVF cycle has failed?
I had bleeding after transfer — does that mean the cycle failed?
What physical changes should I expect after a failed IVF cycle?
How should I handle my emotions immediately after a failed cycle?
What should I do in the first week after receiving a negative result?
What will the clinical review cover when I meet my doctor?
What laboratory and genetic factors might explain IVF failure?
How do I decide whether the problem is fixable or whether to change clinics or consider donor options?
What practical strategies help with emotional recovery after a failed IVF?
Where can I get emotional support specific to IVF failure?
What options exist for a second IVF attempt and how can success rates be improved?
What alternative fertility treatments should I consider after IVF failure?
When is it appropriate to try IVF again?
What if I feel unable to cope or have thoughts of harming myself after a failed IVF?

Author Bio: Neelam Chhagani is an International Surrogacy Expert with 15 years of experience in the fertility and surrogacy domain. As the founder of IVF Conceptions and Complete Surrogacy, she has guided over 4,000 intended parents worldwide on their surrogacy journey to parenthood. Recognized as a trusted authority, she specializes in holistic infertility solutions and third-party reproduction consulting.
Holding an MA in Counselling Psychology and a PGD in Mental Health, Neelam is a proud member of the European Fertility Society (EFS) and the European Society of Human Reproduction and Embryology (ESHRE). She is also a leading surrogacy blogger, providing valuable insights into ethical and practical surrogacy solutions.
Since 2010, committed to supporting ALL family types, Neelam has been passionate about helping intended parents grow their families with compassion, integrity, and a focus on secure and affordable surrogacy options Globally.
Learn more about Neelam:
https://www.ivfconceptions.com/neelam-chhagani-surrogacy-consultant/
https://www.linkedin.com/in/neelam-chhagani-92892229/












I was introduced to Neelam by a friend who worked with Neelam for surrogacy. Neelam is absolutely wonderful. I am a single male and the journey to fatherhood is not that easy. Neelam connected me to a program ideal for my circumstances. She was with me throughout the pregnancy providing advice and guidance along the way. I am so grateful I found her and am thrilled today that I have a beautiful daughter. I highly recommend Neelam to anyone who is on a journey to become a parent. Having a child has changed my world for the better. I wish others success with their own journey and recommend you connect with Neelam to find a path that is best for you.
SA (USA)